That’s not what he said though, he stated there have been 5 times as many deaths. Maybe he misspoke, maybe he misunderstood the information, either way I wanted to address the inaccuracy.
That’s totally fair. I was not intending to suggest you had presented inaccuracies. I just felt that the range of flu deaths and the duration of flu season were two additional details that were important to consider.
Just like it is important to consider that the government was paying doctors more money to list the death a covid-19. So the numbers aren’t even somewhat believeable.
1 Like
The consensus among scientists and public health officials is that the numbers are actually too low rather than too high.
1 Like
Since we talked about this on the last thread I thought this was a worthwhile share. I’m sure some will knock the source but it does credit sources on both sides of the argument.
I was going to bring this up. It has been reported that Nursing homes and hospitals have been claiming Covid with out any real confirmation and in some cases when it’s not.
The CARES Act created relief funding for hospitals and Nursing homes. It has a 20% add-on to be paid for Medicare patients with COVID-19.
I honestly just don’t trust any of the numbers to be remotely accurate.
1 Like
The numbers definitely aren’t accurate. But again, the expert consensus is that they are too low, not too high.
https://www.nationalgeographic.com/science/2020/05/what-we-need-to-find-true-coronavirus-death-toll/


Poor poor assumptions brother…
I hope you never get robbed as you will never be able to defend yourself- nice choice to be totally vulnerable …
Hiding your fear behind poor choices like no locks and guns… your choice thought and mine is not to be told what to do!
Yep! Piss poor data… been saying it the whole time… data spun for an agenda… period
LOL, you’re a gem. Tonight when you turn the lights off make sure it’s cocked and loaded. I’m “hiding” in plain sight and you’re a cowering victim of your circumstances. Yep, still wearing my mask when needed, not at all today because it wasn’t, but realistic and more than caring about others when I need to. Really sad that you still have no care about anyone but yourself.
The problem with that model is that short of super high end SCUBA or gas masks, nothing is 60% effective at reducing the transmissibility of viruses (which is VASTLY more difficult than reducing the # of detectable virus by 60%).
Because of the way that microorganisms and viruses reproduce, you need to have a 3+ log (99.9%) reduction in input or output to have any meaningful reduction in contamination. My background is more in bacterial disinfection than virus deactivation, but I know EPA rules are that to claim bacterial disinfection, you need to demonstrate a 6-log reduction (99.9999%) reduction in 10 minutes. Even when we weren’t looking to meet those high standards, anything less than a 4-log reduction (99.99%) was deemed ineffective.
This is what irritates me about claims that masks do anything, especially from folks who “believe in science”. I’m not saying this to you specifically - you actually come across as at least somewhat open to data - but I’m goddamned sick and tired of being lectured by people who are way less informed than I am about the scientific method and data analysis.
Let’s take, for example, the paper that you linked in a previous thread.
https://www.preprints.org/manuscript/202004.0203/v2/download
It took me a week to get to really reading it and the underlying references, and it frankly infuriated me how bad this paper is. They ignore the studies to come to a conclusion of essentially, “we think this might work”.
I know this is probably tedious for most people, but let’s break the key sections of this paper down:
2. Transmission Characteristics of COVID-19 - This is a bunch of theoretical and modeling that is not emperical. Lots of references to make it look “sciencey”. Maybe a little bit of background for the uninformed, regarding physical properties of droplet size and the like, but nothing regarding mask efficacy.
3. Ingress: Filtering Capability of Masks - The authors waste several paragraphs talking theoretically about droplet blocking (which other studies already show doesn’t correlate to anything) before they cite the studies that show that cloth masks don’t do anything meaningful (MacIntyre) and the ones that show that even N95 masks can’t protect any better than a surgical mask (Young and Radonovich). They didn’t show any studies about surgical masks vs. no mask, but the trend in the data is that at best surgical masks might be minimally effective. However, they present no evidence to support even that tepid conclusion.
4. Egress: Masks for Source Control - Again, they bloviate for paragraphs about droplets before getting to the studies that actually have meaningful data. And this is what really grinds my gears. First, they take the recent Korean study (Bae) and totally misconstrue the results. This is one of the studies that I linked in that earlier thread, and it shows essentially no difference (<1 log) between COVID patients coughing into petri dishes with masks (surgical and N95) and no mask. The authors in your paper actually try to claim that this study supports the efficacy of masks, when the consensus is that this study shows the exact oppositie of that.
They also reference one study that does sort of support masks (Leung), but that study has really questionable data. They did a similar study to Bae, except with a rhinovirus, a flu virus, and a coronavirus (not COVID-19). The main results table is below:
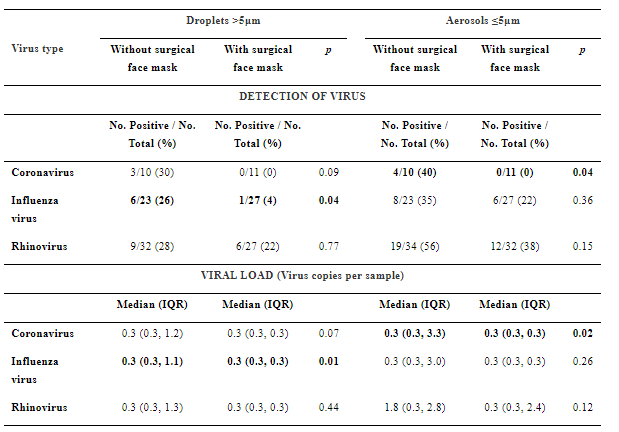
If the data are taken at face value, you might be able to say that a surgical mask somehow is effective at reducing the coronavirus tested while not being meaningfully effective against the flu and rhinorvirus.
I don’t buy it. What is far more logical, and supported by the data, is that this study is flawed because of a detection mechanism that is not sensitive enough. It’s only positively detecting virus in 37% of the non-masked tests. That’s not nearly high enough to have much confidence in their testing system. What likely happened is that the very minor reduction (<1 log) of virus that masks seem to provide (as demonstrated by Bae) reduced the viral load below the detection limit of the apparatus used by Leung.
And that’s it for the real studies. The paper then goes on to make a bunch of hypothetical assumptions about how effective masks could be (after not doing a damn thing to demonstrate effectiveness).
The flip side is that there are numerous other studies that show that masks aren’t effective for public health, many linked in this “study” that’s more of a data-supported opinion piece: https://www.researchgate.net/publication/340570735_Masks_Don’t_Work_A_review_of_science_relevant_to_COVID-19_social_policy
The bottom line is that the vast bulk of the evidence is that masks don’t work. If you want to wear one, fine. Just like if you want to take massive doses of vitamin D or whatever. I don’t care. But stop trying to make me wear one just to comply with idiotic rules made by uniformed idiots, and don’t think for a minute that you’re more informed than me on the topic (the general “you”, not you specifically CuriousHusker).
3 Likes
And now they can’t even agree about when to wear the masks we - who are not in denial of their underlying fear of no control and death - already knew sucked and were not effective at all…
And you don’t care about your own family… no locked door for your family? No firearms in your house to protect them? Now that’s hypocrisy at your best!! Keep it up… you keep failing and failing… prayers for you brother
1 Like
Thank you. That was an incredibly detailed and well informed response. I greatly appreciate you taking the time to share it with us.
Do you know what type of masks are typically used by Japanese citizens? Dr. Gottleib specifically mentioned them as an example of the effects of wearing higher quality masks. I wish he would’ve mentioned which study he was reference but he did not. I’ve always found Dr. Gottleib to be well informed, grounded and non-political. I actually stumped for him being a logical head of the task force a few months ago. Perhaps some of my faith in him is misplaced.
The Czech Republic also has credited their mandatory face mask policy as a reason for their success with the virus.
I’m guessing that Dr. Gawande (below), who I’ve been impressed with when I’ve seen him on TV, is referencing the same study.
I of course have no expertise on this, or any other health matter. As much as anything I tend to follow those experts that I know and/or trust because of credentials. When there is significant consensus I generally adopt that line of thinking. Some here think that makes me a sheep. I happen to think it means I know my limitations and try my best as a lay person to compensate by following those I seek trustworthy.
There’s likely some undercounting from early on, before the focus of the universe was on this single disease, but there’s increasing evidence that in the US, at least, overcounting is far more common. From discounting co-morbidities (people dying with COVID rather than from COVID) to outright fraud, there are many examples.
This makes sense, given that there are financial incentives for counting a death as COVID paired with the fact that many hospital systems are in financial distress because of the unnecessary bans on procedures not COVID-related. While not a justification for that behavior, it is certainly a rational explanation.
It seems obvious that in countries with little health care infrastructure that confirmed counts are undoubtedly low. It also wouldn’t surprise me to see the opposite bias to the US in countries like Germany, where the political pressure and culture is to want to be successful against this disease.
Again, i have no expertise in the matter so I can’t personally vouch for either aside of the argument. But it’s pretty clear that there is a consensus amongst experts that the totals are likely undercounted not over over-counted.
The issue of who died with Covid-19 vs. who died of Covid-19 proves to be a challenge. I found this to be a Interesting article on the topic matter.
1 Like
Good read. Looks to be an easily identifiable cause when conducting post-mortem.
“Most of the cases are pretty straightforward,” Fowkes told Live Science. “The lungs are usually so severely involved with pathology, so they are two to three times or more the normal weight of a normal lung"
It goes on to cover deaths at home. The excess death data will be telling, but definitely not of the conspiratorial variety that is being pushed.
2 Likes
Ah, if I’m not armed I’m a hypocrite? Can you show me in the Old or New Testament where anyone said that? Nope, you are the hypocrite claiming your religion will keep you safe from the virus but mine won’t keep me safe w/o locked doors and guns. God thinks you need to spend more time reading the bible if you are going to use him as an excuse for your irresponsibility to your fellow man.
Psalm 4:8, “In peace I will lie down and sleep, for you alone, O Lord, will keep me safe.”
I believe CV numbers are skewed in a lot of ways, some on purpose: malpractice, mislabeled deaths, misplacement of patients etc.
But, CV is new and there wasn’t a lot out there on how to treat it which was cause for part of the issues above. Will a vaccine help with some deaths for those that want to get it? How long will it take to figure out the best way to treat it? Flu has been around forever and it has an annual vaccine and ways it is to be treated but is still quite deadly considering.
One friend of mine got it at 34. His Labs were awful when he went in with CV, 6’3" nearly 400 lbs and known high blood pressure. Wasn’t expected to make it. He was on the vent for 10 days total. His mother and wife pushed the hospital to give hydroxychloroquine he started seeing improvements but they can’t say if it was directly related to that or not or if it was something they could have done sooner or not needed. He ended up losing 90 lbs. He was allowed to go home after 2 or 3 negative tests and so many hours(48?).
A couple other friends of mine got it. Both in their late 40s and live near DET. One is little overweight, not sure if he smokes or not. He got it and they sent him home because of his age. His oxygen got down to the low-mid 70s at home and he never went back in. He recovered but said he could hardly move or breathe for 4 days. He’s back to work now. The other buddy of mine swore he had it in January was tested negative for any flu. He’s an avid smoker and that it felt like he was dying at times but no one else in his house even had a sniffle. He recently had his antibodies tested to find out he had it.
My wife and other ER nurses are saying to avoid the vents as long as physically possible. In some places hospitals were putting patients on vents too soon.
I thought this was interesting:
4 Likes